Treatment and Rehab at the Foot for Plantar Fasciitis

Treatment and rehab for plantar fasciitis can involve everything from foot, ankle, hip, and core based on your individual presentation. We will start from the bottom and move on up in an succeeding blog.
The Foot and Plantar Fasciitis
There are twenty-six bones, thirty joints and more than one-hundred muscles, tendons and ligaments that make up each foot and work together to provide balance and support for the entire body. In our opinion, even outside of plantar fasciitis the foot does not get enough credit or look at it for its contribution to entire body function.
As talked about in the previous blog, treatment and rehab for foot that is too mobile and foot that is not mobile is completely different with plantar fasciitis. Sometimes based on the assessment we can have a combination and will have to do things in both categories.
- Hypermobile foot: for this we are going to look at stability (controlling the range of motion) of the foot. Range of motion like pronation is not bad, but if we are not able to control it effectively than that can lead to a problem. Specifically, with the feet controlling pronation and controlling the speed of which the toes move upward during the propulsive period of running and walking.
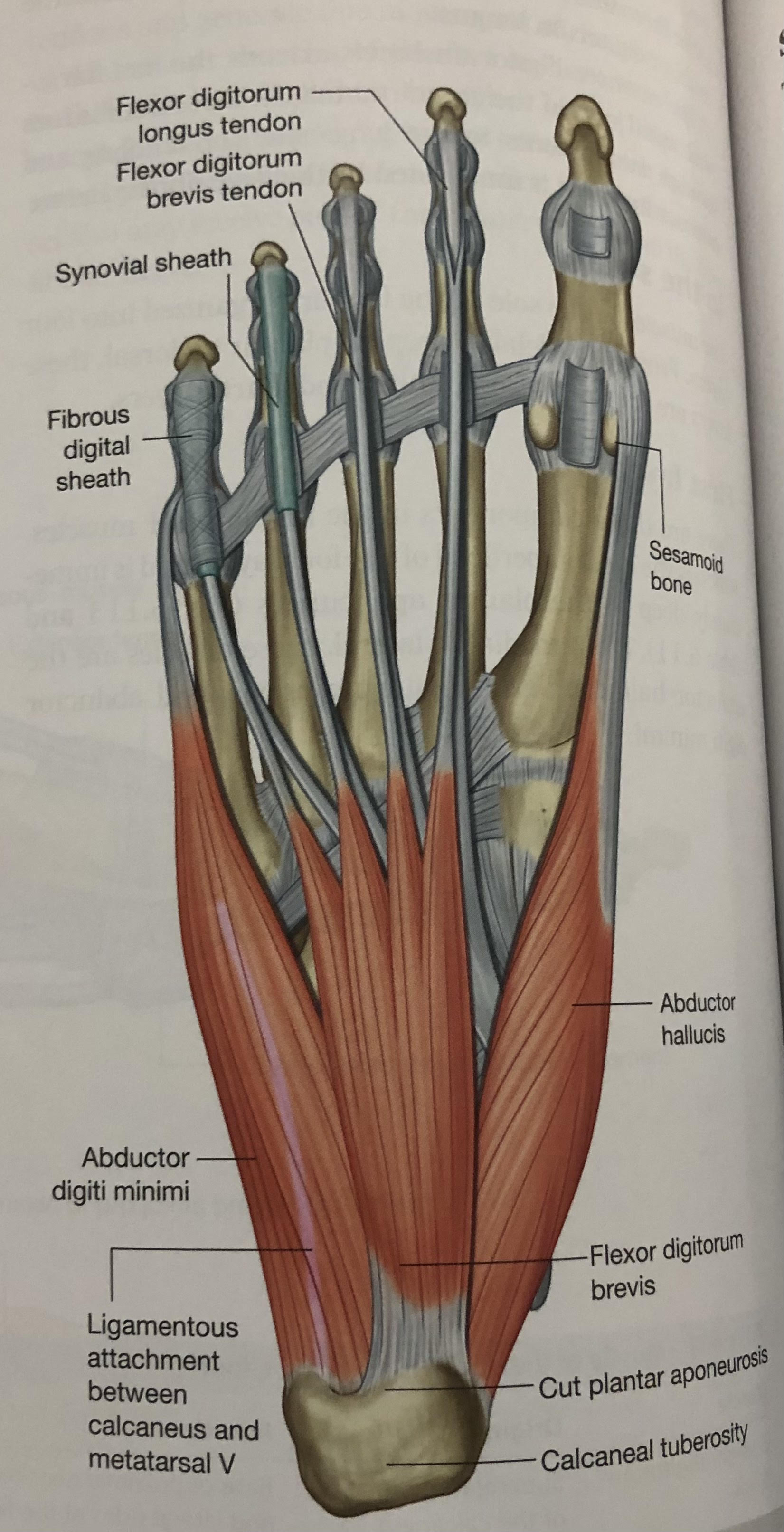
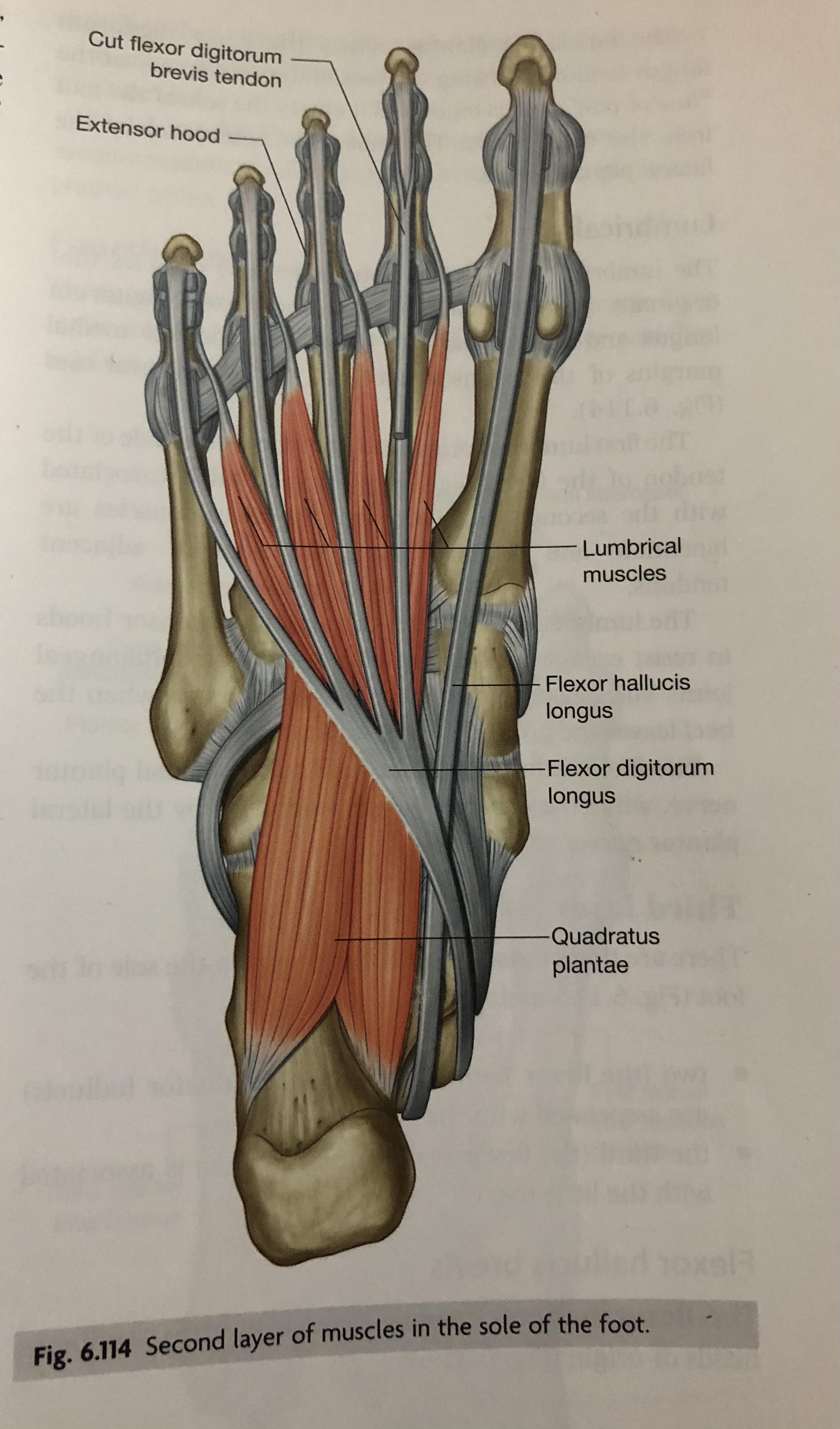
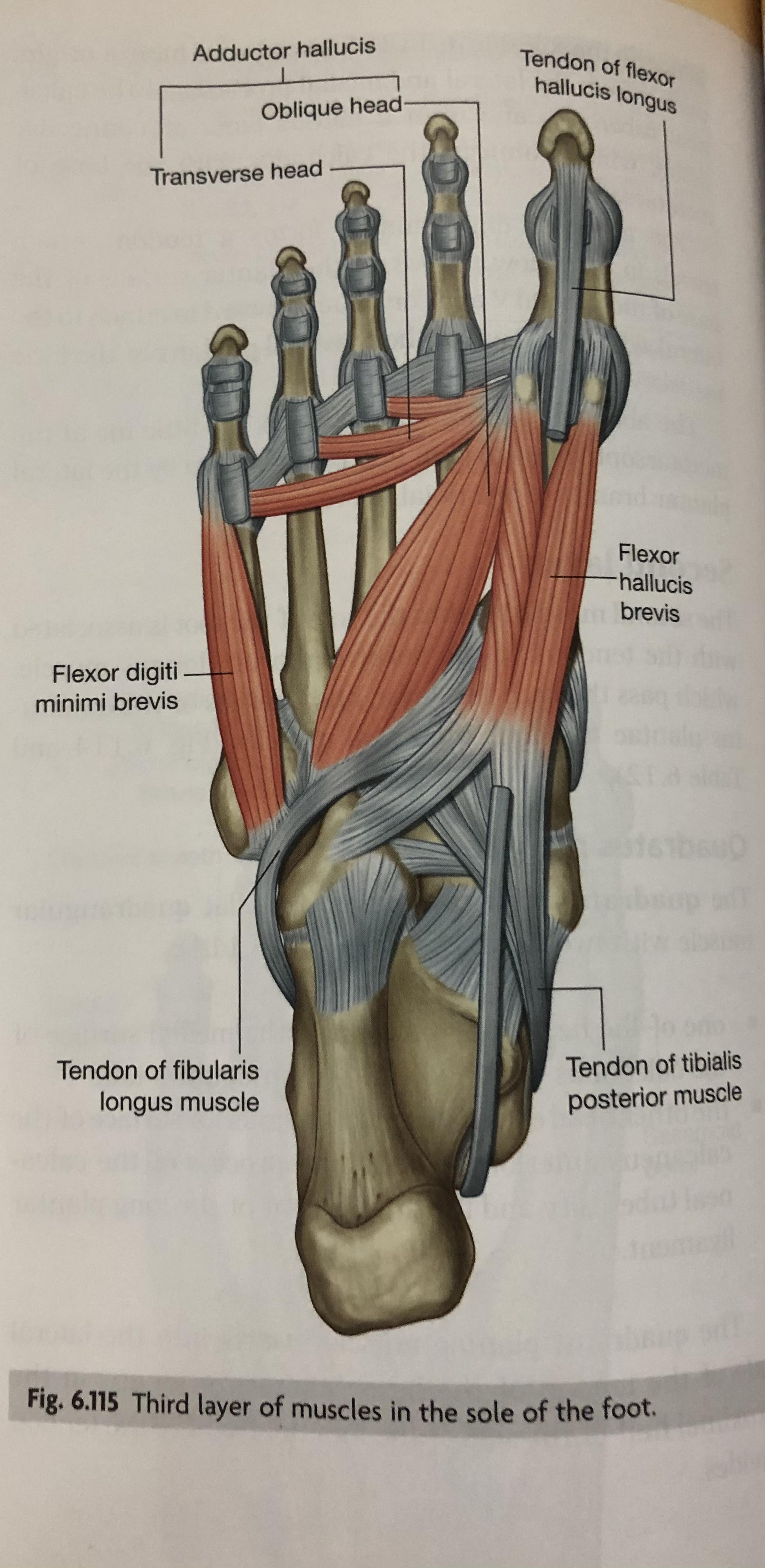
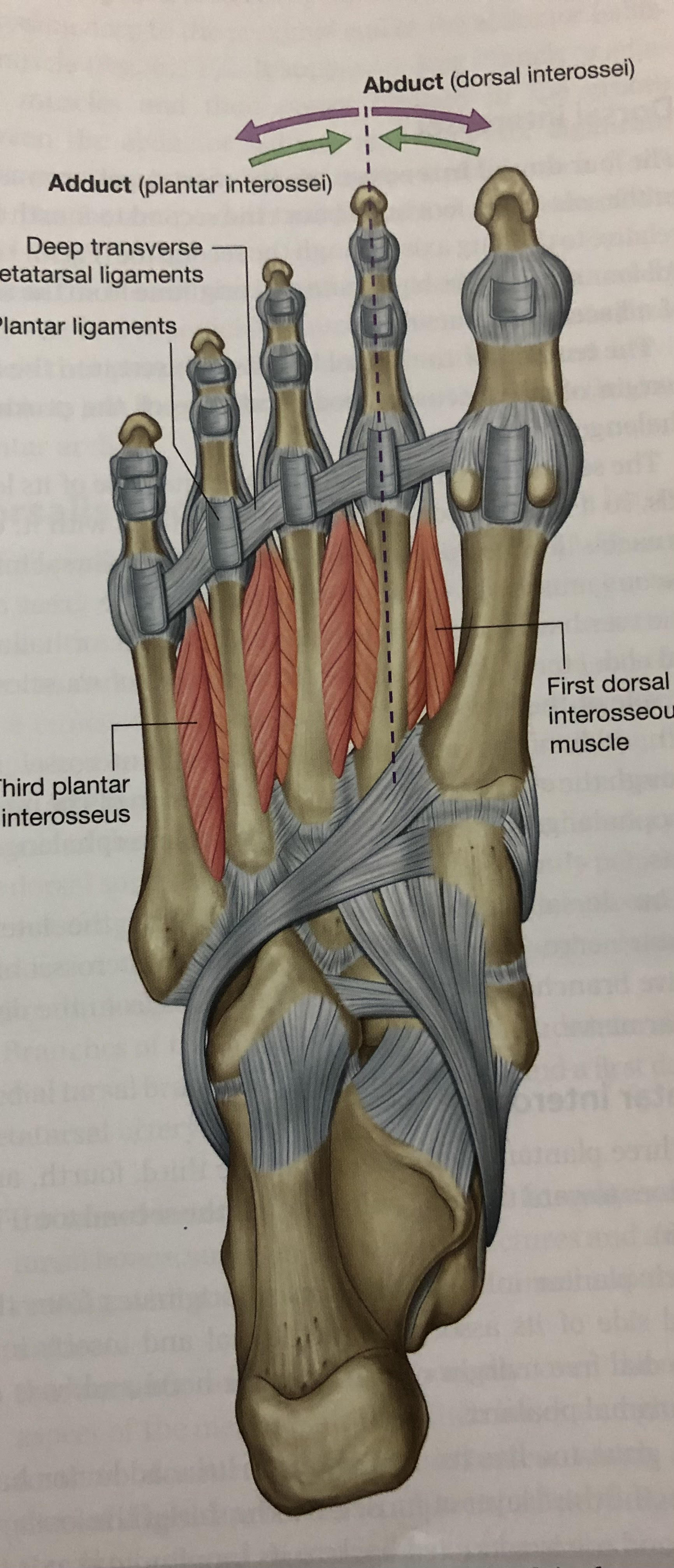
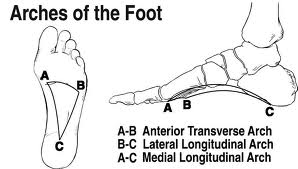
- Treatment for this is going be more focused on strengthening muscles in the foot that control the arch of the foot moving into pronation and muscles that control movement of the toes. Focusing on muscles like the tibialis posterior which is the main muscle that controls the arch and the smaller intrinsic (meaning deeper) muscles in the foot that are responsible for fine motor actions of the foot. There are four layers (photo of each layer posted below) included in these intrinsic muscles that act in coordination to stabilize the arches of the foot and individually to control movement of the toes. There are few “simple” tests leading to exercises we can do in office to test the vitally important function of these muscles. All foot rehab will be focused on maintaining, strengthening, and loading the “tripod” function as seen in the arches photo below.
-
- Clinic treatment: To help with pain, in clinic, we love finding a repeated movement (McKenzie method) you can do to help decrease pain and sensitivity yourself in the short term. We can also do dry needling or instrument assisted soft tissue manipulation (IASTM) to help decrease trigger points and tension. Kinesiology taping can also be great to help decrease sensitivity.
- Hypomobile foot: for this we are going to look at increasing range of motion through the foot. Through assessment we will see if the mobility restriction is more from the joint or the muscle.
- One of the first things we will look at is big toe mobility as we need at minimum 45 degrees of extension range of motion (big toe going up towards the top of your foot) in the normal propulsion of walking and running. Sounds wild that the big toe can have a big effect on overall body mechanics, but it plays a huge roll since the plantar fascia connects to the base of it. Because of this when it has limited mobility, it can cause extra strain going up the chain of the body because you will not be able to effectively roll through the foot and big toe as you walk. Leading you to have to roll the foot more outward to accomplish the push off phase of gait. Next, we would look at the joints in the mid-foot and making sure there are no restrictions to allow proper pronation and supination as we go through the walking and running gait cycle.
- Clinic Treatment: In clinic, for pain we will focus on most of the same things as before with some additions: adjusting to open up both the big toe and midfoot, McKenzie exercises, IASTM, dry needling, cupping, and taping. Rehab at home will be focused on exercises that increase and reinforce the range of motion that we have gained.
Next blog we will focus on the ankle, hip, and core and how function at each can tie into plantar fasciitis!
References: Drake, R. L., Vogl, W., Mitchell, A. W. M., & Gray, H. (2005). Gray's anatomy for students. Philadelphia: Elsevier/Churchill Livingstone.
